80 year old male with CKD
Final exam case report - Long case.
Name: A. Rishi koundinya
Hall ticket number: 1701006010
Batch - 2017
"This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box
Dt. 06.06.2022
Chief complaints
80 years old male resident of marrigudem, agriculture labourer by occupation came to OPD with the chief complaints of
fever - since 3 days
An episode of vomiting 2 days back
Decreased urine output associated with burning micturition since - since 2 days
History of presenting illness
patient is apparently asymptomatic 3 days back.
He has fever :
insidious in onset
gradually progressive
with no diurnal variations
Relieved on medication
Associated with chills, rigors and generalised body pains. It is not associated with cough, cold, shortness of breathe, night sweats.
Associated with an episode of vomiting 2 days back which is of only food which is non bilious and not foul smelling and colour is same as the food colour.
There is burning micturition which is experienced at the start of the urinary flow and relieved after the urination and decreased urine output since 2 days which is not associated with any hematuria.
Past history

He was with similar complaints in the past 10years ago, then he consulted a local doctor and relieved on medication (may be antibiotics). And there is continuation of such episodes then refered to higher hospital and diagnosed with renal problem (AKI) which was treated with dialysis once and given some diuretics as he is suffering from oliguria.
He has a recurrent episodes of fever with burning micturition later also.
He is known case of hypertension since 24years. Not a known case of diabetes, tuberculosis,asthma and epilepsy.
Surgical history
He underwent a nephrectomy surgery 27yrs ago donated to his brother.
Personal history
Appetite - normal
Diet- mixed
Sleep - adequate
Bowel - regular
Bladder - oliguria since 2 days, associated with burning micturition, feeling of incomplete voiding.
Allergies- none
Addiction- 3 beedi/ day from 27yrs of age
Alcohol- occasionally
Stopped both alcohol and smoking after the nephrectomy surgery.
General examination
Patient is conscious, coherent, co operative and well oriented to time, place, and person moderately build and nourished.


There is pallor and pedal edema , but no icterus , cyanosis,clubbing, lymphadenopathy.
Vitals: Febrile 99.2F

Bp- 150/90 mmHg ( on medication)
Pulse rate - 76 BPM
Systemic examination
- cardio vascular examination
No visible pulsations, scars, engorged veins. No rise in jvp
Apex beat is felt at 5 ics medial to mid clavicular line.
S1 S2 heard . No murmurs.
- Respiratory system
Shape of chest is elliptical, b/l symmetrical.
Trachea is central. Expansion of chest is symmetrical
Bilateral Airway E - positive
- Per abdomen examination
No visible pulsations and scars swellings.
Soft, non tender, no organo megaley.
Umbilicus is inverted.
CNS EXAMINATION:
Conscious
Speech normal
No signs of meningeal irritation
Cranial nerves: normal
Sensory system: normal
Motor system: normal
Reflexes: Right. Left.
Biceps. ++. ++
Triceps. ++. ++
Supinator ++. ++
Knee. ++. ++
Ankle ++. ++
Gait: normal




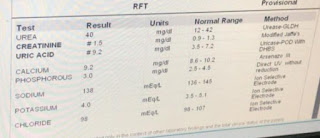
Investigations.







Treatment:
Inj. Piptaz -2.25gm/tid
Tab. Lasix -40ug/po/ bd
Tab. Zofer -4mg/po/ sos
Tab. Dolo -650/ po/ sos
Tab. Pan 40mg /po/ od
Nebi. Duolin and Budecort 6hrly
Syr. Mucaine gel 15ml/po/ bd before meal 15min
Syrup. Cremaffin 15ml/po/ sos.










Comments
Post a Comment