50 year old man with ascites
Final case report - Short case
Name - A. Rishi koundinya
Hall ticket number- 1701006010
Batch - 2017
"This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box"
Chief complaints
50 year old male, farmer by occupation, resident of Pochampally, came to Medicine OPD with complaints of :
* Distended abdomen since 7 days
* Pain abdomen since 7 days
* Pedal edema since 5 days
* Breathlessness since 4 days.
History of presenting illness
The patient was apparently asymptomatic 6 months ago when he developed jaundice and was treated at a private practitioner.
Later he developed abdominal distension about 7 days ago - insidious in onset, gradually progressive to the present size - associated with
Pain in epigastric and right hypocondrium - colicky type.
Fever - high grade, not associated with chills and rigor, decreased on medication, No night sweats.
Not associated with Nausea, vomiting, loose stools

There was pedal edema
Gradually progressive
Pitting type
Bilateral
Below knees
Increases during the day - maximum at evening.
No local rise of temperature and tenderness
Grade 2
Not relived on rest

He also complained of shortness of breath since 4 days - MRC grade 4
Insidious in onset
Gradually progressive
Agrevated on eating and lying down ; No relieving factors
No PND
No cough/sputum/hemoptysis
No chest pain
No wheezing
Patient is a known alcoholic since 20 years. Ascites increased after his last drink on 29th May, 2022. Alcohol- 2 times a week, 180 ml.
Past history
No history of similar complaints in the past
Medical history- not a known case of DM, HTN, TB, Epilepsy, Asthma, CAD
Surgical history - not significant
Personal history
Diet - mixed
Appetite- reduced since 7 days
Sleep - disturbed
Bowel - regular
Bladder - oliguria since 2 days, no burning micturition, feeling of incomplete voiding.
Allergies- none
Addictions - Beedi - 8-10/day since 20 years ;
- Alcohol - Toddy - 1 bottle, 2 times a week, since 20 years;
- Whiskey-180 ml, 2 times a week, since 5 years.
- Last alcohol intake - 29th May, 2022.
General examination
Patient is conscious, coherent and co-operative.
Examined in a well lit room
Moderately built and nourished
Icterus - present
Pedal edema - present - bilateral pitting type, grade 2
No pallor, cyanosis, clubbing, lymphoedenopathy.


Vitals :
Temperature- febrile
Respiratory rate - 16cpm
Pulse rate - 101 bpm
BP - 120/80 mm Hg.
Systemic examination:
CVS : S1 S2 heard, no murmurs
Respiratory system : normal vesicular breath sounds heard.
Abdominal examination
INSPECTION :
Shape of abdomen- distended
Umblicus - everted
Movements of abdominal wall - moves with respiration
Skin is smooth and shiny;
No scars, sinuses, distended veins, striae.
PALPATION :
Local rise of temperature present.
Tenderness present - epigastrium.
Tense abdomen
Guarding present
Rigidity absent
Fluid thrill positive
Liver not palpable
Spleen not palpable
Kidneys not palpable
Lymph nodes not palpable
PERCUSSION:
Liver span : not detectable
Fluid thrill: felt
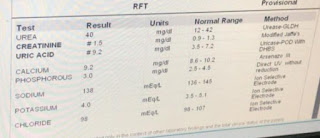
Investigations
Serology:
HIV - negative
HCV - negative
HBsAg - negative













PROVISIONAL DIAGNOSIS:
Liver failure with ascites.
TREATMENT:
Syp. Lactose 15ml TID
Abdominal girth charting - 4th hourly
Fluid restrictriction less than 1L per day
Salt restriction less than 2 gms per day



Comments
Post a Comment